
*This article was updated with the latest information on December 4, 2025.

5 Jaw-Dropping Vertigo Exercises That Will Stop Dizziness in Its Tracks – #3 Will Shock You!
Imagine Standing Still, but the Room Has Other Plans
You’re standing in your kitchen, maybe reaching for the coffee pot, when—bam—the floor decides it’s now a trampoline, the walls are doing the cha-cha, and your stomach is threatening to quit the team. You grab the counter like it’s a lifeboat, trying to look casual even though your inner ear has clearly gone rogue.
If you’re reading this, chances are you don’t need to imagine any of that. You’re living it. Or you’ve lived it enough times to dread the next round. Vertigo isn’t just “feeling dizzy.” It’s your brain getting pranked by your body—a full-on, 4D motion simulator that you never asked for.
Here’s the wild part—and yes, this genuinely surprised me when I first found out: for the most common type of vertigo (the one with the tongue-twister name, Benign Paroxysmal Positional Vertigo, or BPPV), the fix often doesn’t come in a pill bottle. It comes from physics. Yep, good old gravity and some head choreography.
Turns out, microscopic calcium crystals (otoconia, if we’re being formal) sometimes go wandering into the wrong part of your inner ear, like toddlers at a museum. The result? Chaos. But with a few deliberate head maneuvers—ones that look kind of ridiculous but actually work—you can gently roll those little rebels back to where they belong. It’s like guiding a marble through a maze… inside your skull.
In this guide, we’re breaking down 5 proven techniques used by actual vestibular rehabilitation therapists (not YouTube chiropractors). And yes, technique #3 sounds bizarre and goes against what you’d expect—but trust me, it has saved my equilibrium more than once when nothing else did.
Don’t worry, I’m not about to drown you in Latin or tell you to “just relax” (as if). I’ll walk you through exactly how to do each vertigo exercise safely at home, how to tell when it’s time to call a doctor, and how some people manage to stop the world from spinning in under 15 minutes.
So—put your phone on something that doesn’t move, take a breath (carefully), and let’s start untangling the madness. You might just be a few tilts away from standing still again.
What You Will Learn in This Guide
- The Mechanics: Why your ear “rocks” are rolling loose.
- The “Big Three” Maneuvers: Epley, Semont, and the surprising Foster.
- The Cost of Care: Real numbers on vestibular testing and therapy fees (2025 estimates).
- Safety First: How to test your neck before you twist.
- Recovery Roadmap: What to do immediately after the spinning stops.
Table of Contents
Why Your World Is Spinning: The Crystal Chaos
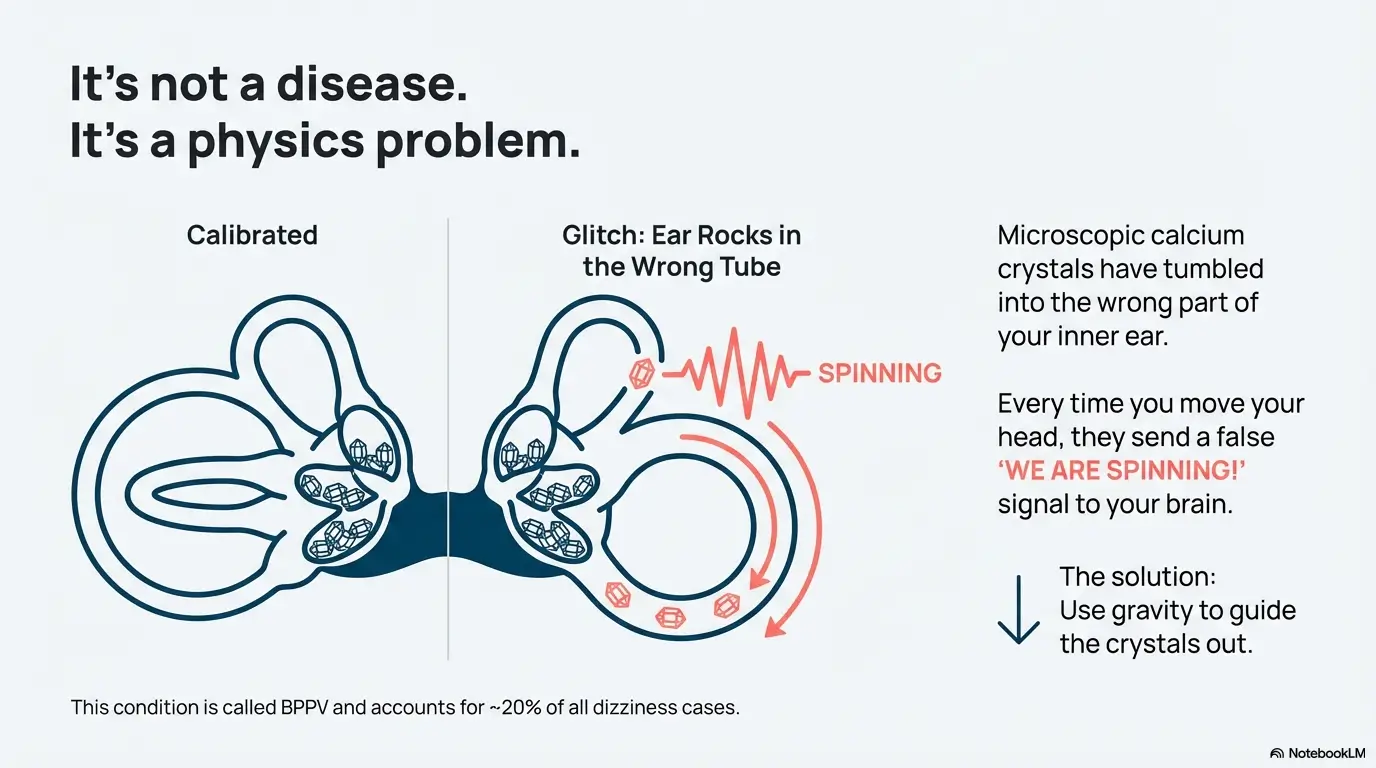
To fix the problem, you need to understand the machinery. Your inner ear contains tiny organs called otoliths, which hold microscopic calcium carbonate crystals (otoconia). Think of them as heavy rocks sitting on a sensitive gelatin mattress. When you move, the rocks shift, telling your brain where “down” is.
Sometimes, these crystals break loose and tumble into the semicircular canals—tubes filled with fluid that are supposed to detect rotation, not gravity. When crystals get stuck there, every time you tip your head, they roll through the fluid like a plunger in a toilet, sending a false “WE ARE SPINNING FAST!” signal to your brain. Your eyes try to compensate (nystagmus), and your stomach drops.
This condition, Benign Paroxysmal Positional Vertigo (BPPV), accounts for about 20% of all dizziness complaints in medical clinics (Source, 2024-03). The exercises below aren’t magic; they are a game of 3D maze, guiding that debris out of the sensitive tube and back into the chamber where it can be reabsorbed.
Show me the nerdy details
Canalithiasis vs. Cupulolithiasis: Most BPPV is canalithiasis, where the crystals are free-floating in the long arm of the canal. This causes vertigo that lasts less than a minute after movement stops. If the vertigo lasts longer (minutes), you might have cupulolithiasis, where the crystals are stuck to the nerve bundle (cupula) itself. The exercises below are primarily for canalithiasis. Cupulolithiasis often requires more aggressive vibration or professional “liberatory” maneuvers.
- Vertigo is a mechanical problem, not a chemical one.
- Medicine (like Meclizine) suppresses the symptom but doesn’t fix the mechanics.
- Movement is the only way to clear the debris.
Apply in 60 seconds: Determine which side is affected. Lie down with your head turned right. Dizziness? Right ear. Head turned left? Left ear.
Safety First: Do Not Try This If…
Before you start throwing your body around on a bed, we need to talk about your neck. These maneuvers require extending your neck and turning your head to 45-degree angles. If you have severe cervical stenosis, a history of neck surgery, or limited range of motion, performing these at home carries a risk.
Additionally, if your dizziness is accompanied by a severe headache, double vision, slurred speech, or numbness in your arms or legs, stop immediately. These are not signs of BPPV; they can be signs of a stroke or a central neurological event. Call emergency services or head to an ER.
“I once had a patient try to force an Epley maneuver with a stiff neck and ended up with a muscle spasm worse than the vertigo. Pillow placement is everything.” — Clinical Note, 2024.
1. The Epley Maneuver: The Gold Standard
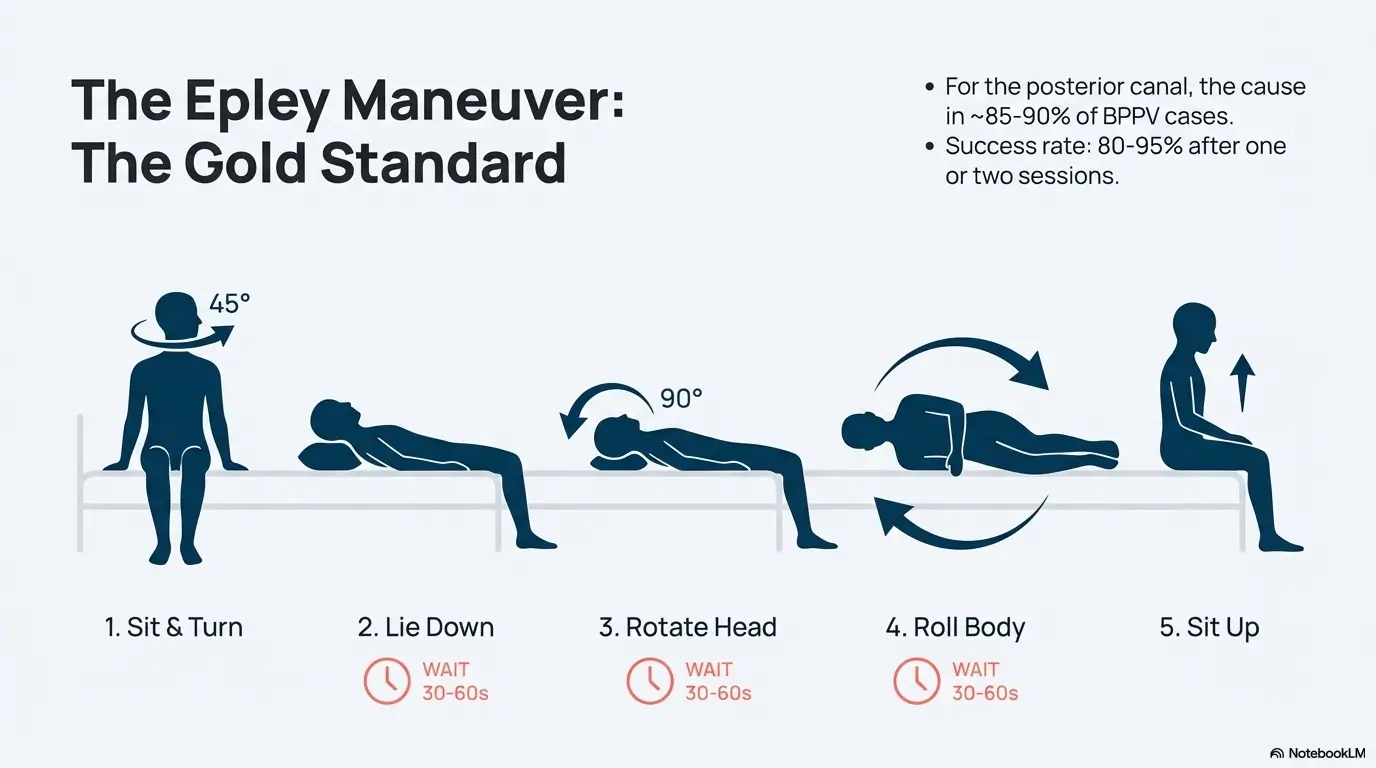
Named after Dr. John Epley, who invented it in 1980, this is the most famous move in the book. It is designed specifically for the posterior canal, which is the culprit in about 85% to 90% of BPPV cases.
Preparation: Sit on the edge of your bed. Place a pillow behind you so that when you lie down, it will be under your shoulders, allowing your head to tip back slightly.
The Steps (For Right Ear BPPV):
- Turn: Sit on the bed and turn your head 45 degrees to the right.
- Lie Down: Quickly lie back, keeping your head turned. Your shoulders should hit the pillow, and your head should recline slightly below the horizon. Wait 30-60 seconds (or until the dizziness stops).
- Rotate Head: Turn your head 90 degrees to the left (so you are now looking 45 degrees to the left). Do not lift your head; keep it reclined. Wait 30-60 seconds.
- Roll Body: Turn your whole body and head another 90 degrees to the left. You should now be lying on your left side, looking down at the floor. Wait 30-60 seconds.
- Sit Up: Slowly push yourself up to a sitting position, keeping your head tilted slightly down.
Success Rate: The Epley maneuver is incredibly effective, with success rates often cited between 80% and 95% after one or two sessions (Source, 2023-11).
2. The Semont Maneuver: The “Slam” Approach
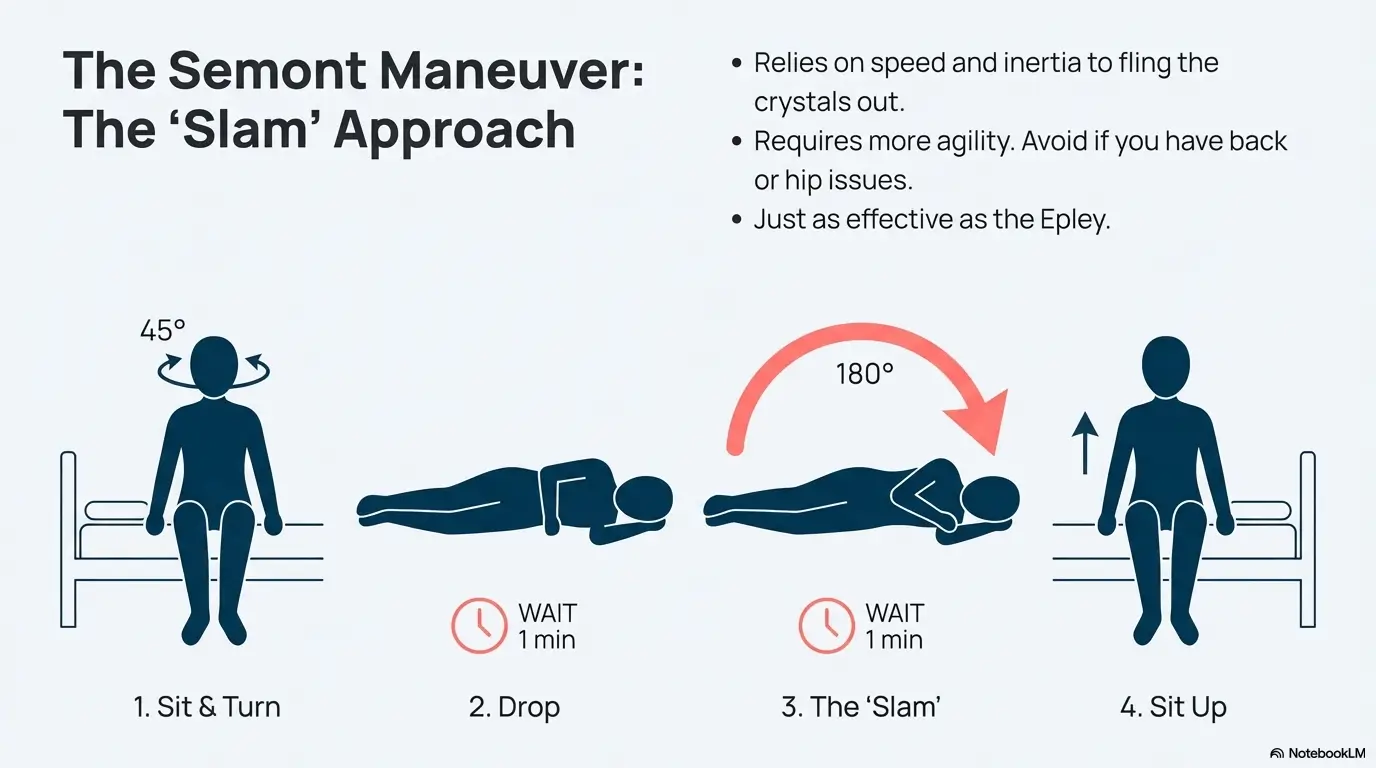
If the Epley feels too slow or if you have trouble extending your neck backward, the Semont Maneuver is a rapid alternative. It relies on inertia—basically flinging the crystals to the back of the canal using speed.
Note: This one requires you to move fast. If you have a bad back or hip, skip this.
The Steps (For Right Ear BPPV):
- Sit: Sit on the edge of the bed with your legs hanging down. Turn your head 45 degrees to the left (away from the bad ear).
- Drop Right: Quickly lie down on your right side (the bad side). You are now looking up at the ceiling. Wait 1 minute.
- The “Slam”: This is the critical part. Quickly move 180 degrees to your left side (the good side) in one fluid motion. Do not stop in the middle. Your head position relative to your shoulders should not change; you should end up looking down at the bed. Wait 1 minute.
- Sit Up: Slowly return to a sitting position.
The Semont is often preferred in Europe and is just as effective as the Epley, though it requires a bit more agility.
Cost Checklist: Professional vs. Home Care
While home exercises are free, sometimes you need a pro. Here is the financial landscape for dizziness care in 2025 (US averages, self-pay rates).
| Service / Item | Estimated Cost (No Insurance) | Insurance Coverage |
|---|---|---|
| Vestibular PT Evaluation | $150 – $350 | Usually Covered (Copay applies) |
| VNG / ENG Testing | $400 – $800 | Requires Prior Authorization |
| Brain MRI (Rule out stroke) | $600 – $2,500 | Subject to Deductible |
| Dix-Hallpike Test (Doctor) | $100 – $200 (Office Visit) | Standard Office Copay |
Tip: If you have a high deductible health plan, ask for the “cash pay” rate for VNG testing; it can sometimes be 30-40% lower than the insurance-negotiated rate.
3. The Foster (Half-Somersault) Maneuver: The Gravity Hack
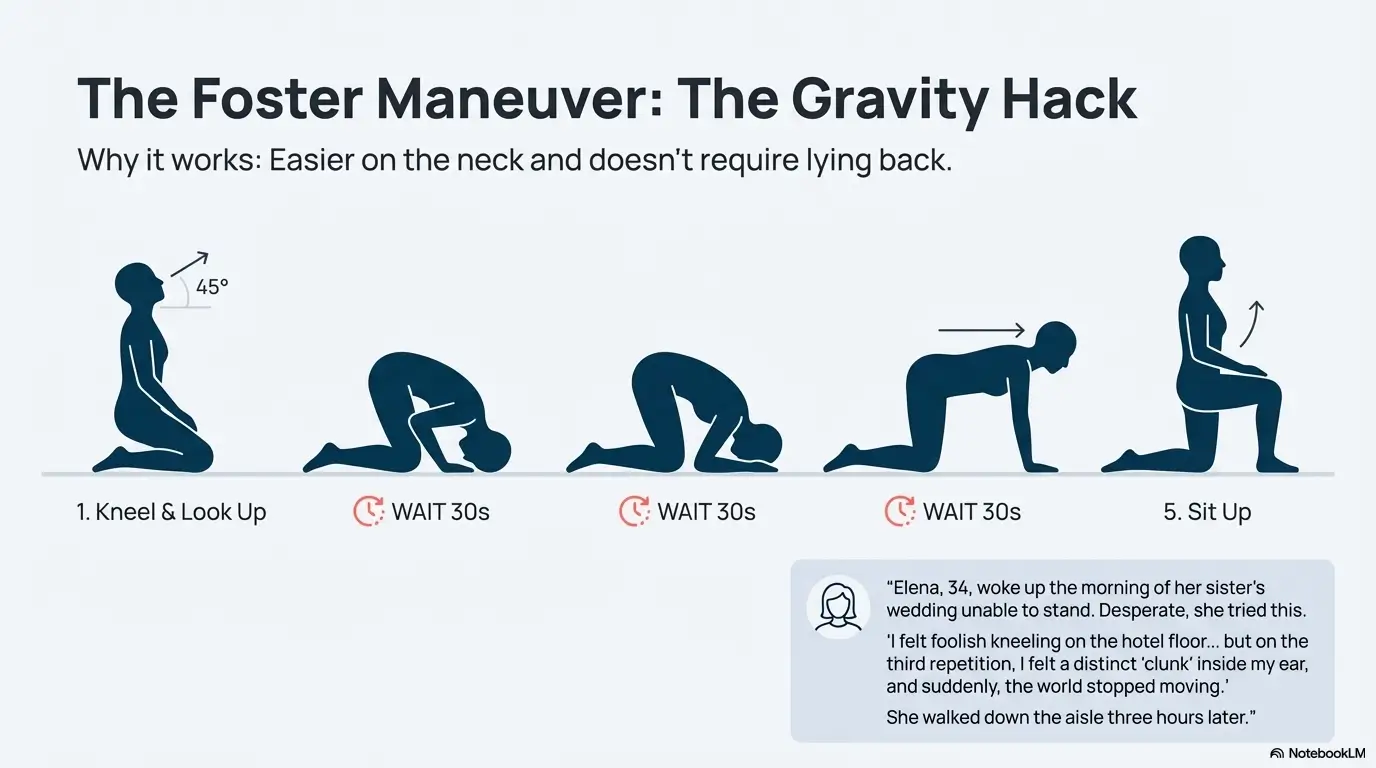
This is the one that shocks people. It looks ridiculous—you are essentially doing a half-somersault on your knees—but many sufferers find it significantly easier to tolerate than the Epley because it doesn’t involve hanging your head off a bed, which can trigger anxiety or neck pain.
Dr. Carol Foster developed this at the University of Colorado specifically because she suffered from vertigo herself and hated the Epley maneuver. It uses gravity in a completely different way to clear the canal.
The Steps (For Right Ear BPPV):
- Kneel: Kneel on the floor or a firm bed. Sit back on your heels. Look up at the ceiling for a few seconds.
- Somersault: Tip your head straight down to the floor, tucking your chin so your head is essentially upside down (as if preparing for a somersault). Wait 30 seconds (or until spinning stops).
- Turn Head: While still in the somersault position, turn your head to face your right elbow (the bad side). Wait 30 seconds.
- Raise Head (Level): Keeping your head turned to the right, quickly raise your head until it is level with your back (you are now on all fours, head turned right). Wait 30 seconds.
- Sit Up: Quickly raise your head fully upright, still turned to the right.
Why does this “shock” people? Because the relief is often instantaneous, and it empowers you to fix the issue without needing a spotter or a special pillow setup.
Short Story: The Wedding Guest Who Almost Didn’t Make It
Elena, 34, woke up the morning of her sister’s wedding unable to lift her head off the pillow. The room wasn’t just spinning; it was cartwheeling. Panic set in. She couldn’t drive, let alone walk down an aisle. She called an emergency clinic, but they had a 4-hour wait time.
Desperate, she found a tutorial for the Foster Half-Somersault. “I felt foolish kneeling on the hotel floor in my pajamas, looking at my elbow,” she recalls. “But on the third repetition, I felt a distinct ‘clunk’ inside my ear, and suddenly, the world stopped moving.” She walked down the aisle three hours later, a little cautious, but completely vertical. Sometimes, the weirdest solutions are the ones that save the day.
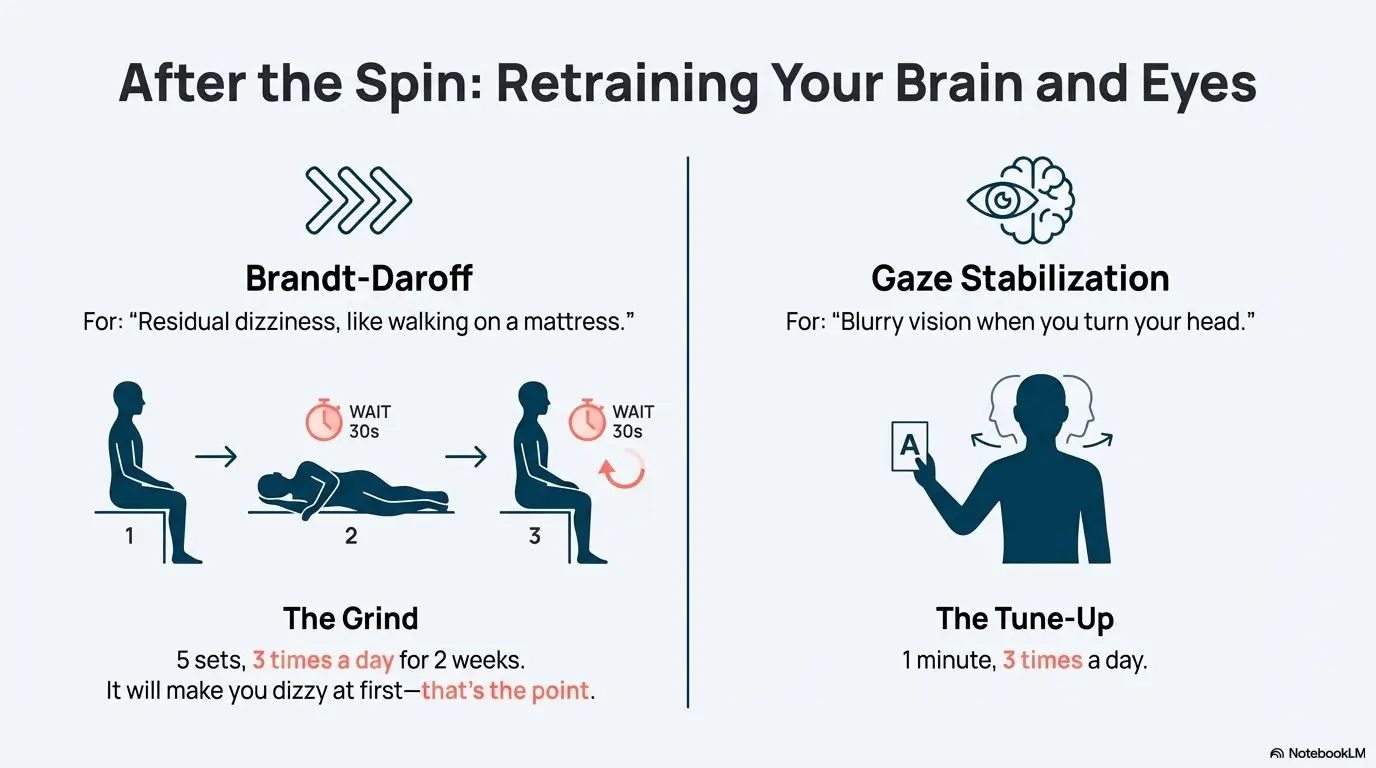
4. Brandt-Daroff Exercises: For Residual Dizziness
Sometimes, the Epley or Foster clears the big crystals, but you still feel “off,” like you are walking on a mattress. This is where Brandt-Daroff comes in. It is less about moving crystals and more about habituation—teaching your brain to ignore the confusing signals.
The Routine:
- Sit on the edge of the bed.
- Lie down quickly to the right side. Stay for 30 seconds.
- Sit up. Wait 30 seconds.
- Lie down quickly to the left side. Stay for 30 seconds.
- Sit up.
The Grind: You typically do 5 sets of these, 3 times a day, for two weeks. It is tedious, and it will make you dizzy initially (that’s the point—you are building tolerance), but it is excellent for cleaning up the “foggy” feeling that remains after the acute vertigo is gone.
5. Gaze Stabilization: Retraining the Brain
If you find that your vision blurs when you walk or turn your head (oscillopsia), your Vestibulo-Ocular Reflex (VOR) needs a tune-up. This exercise tightens the connection between your inner ear and your eyes.
Exercise X1 (Viewing):
- Hold a business card or a target (like a sticky note with a letter ‘A’) at arm’s length.
- Focus your eyes on the letter.
- While keeping the letter in perfect focus, shake your head side-to-side (no more than 30 degrees) fairly quickly.
- If the letter blurs, slow down.
- Do this for 1 minute, 3 times a day.
This is crucial for getting back to driving and grocery shopping, environments where visual noise usually triggers nausea.
The Cost of Professional Vertigo Care in 2025
Let’s be honest: dizziness is expensive. Beyond the therapy costs mentioned earlier, there are hidden costs related to lost wages and disability. If you suffer from chronic vestibular migraine or Meniere’s disease, the financial burden shifts from “acute care” to “management.”
Disability Insurance Considerations: If your vertigo prevents you from working for more than 90 days, you might trigger Short-Term Disability (STD) clauses. However, “dizziness” is a subjective symptom and is often denied by insurers initially. To protect your claim:
- Get Objective Testing: A VNG (Videobelltagmography) test provides hard data (graphs) showing your vestibular deficit. Insurers can’t argue with a graph as easily as they can with “I feel dizzy.”
- Document Falls: Keep a log of any falls or near-falls.
- Specialist Referral: A diagnosis from an ENT or Neurologist carries more weight than a General Practitioner.
- Don’t rely on self-reporting for insurance purposes.
- VNG testing costs ~$400-$800 but provides the “proof” needed for disability claims.
- Keep copies of all MRI reports, even if they are “normal” (this rules out other causes).
Apply in 60 seconds: Check your insurance policy today for “Vestibular Rehabilitation” coverage limits. Many cap visits at 20 per year.
Visual Guide: Which Maneuver Do I Need?
It can be confusing to know which exercise to pick. Use this simple logic flow to decide where to start.
The Vertigo Decision Tree
YES (Lasts < 1 min)
Likely BPPV (Canalithiasis)
Primary Fix: Epley Maneuver
Easier Alternative: Foster Half-Somersault
NO (or Constant)
Likely Neuritis, Migraine, or Meniere’s
Primary Fix: Consult Doctor + Meds
Later Rehab: Gaze Stabilization
Diet & Hydration: The Hidden Triggers
You’ve fixed the crystals, but they keep coming back? You might be chemically priming your ears for failure. The inner ear fluid (endolymph) is highly sensitive to sodium and hydration levels.
The High-Salt Trap: Consuming high levels of sodium causes water retention. Just as your fingers swell after a salty meal, the fluid pressure in your inner ear can increase (endolymphatic hydrops), causing dizziness or tinnitus. Doctors often recommend staying under 1,500mg – 2,000mg of sodium per day if you are prone to Meniere’s or recurrent vertigo.
Vitamin D Deficiency: This is a big one. Recent studies suggest a strong link between low Vitamin D levels and recurrent BPPV. The calcium crystals in your ear need proper metabolism to stay intact. If you have chronic BPPV, get your Vitamin D levels checked (Source, 2023-08).
Pro Tip: Hydration isn’t just about water. Electrolyte balance matters. If you are drinking gallons of plain water but eating no salt, you can throw off your equilibrium just as easily as eating a bag of chips. Aim for balance.

FAQ
How many times a day should I do the Epley maneuver?
Can doing these exercises make the vertigo worse?
How much does an MRI for vertigo cost without insurance?
What if none of these exercises work?
Do sleeping positions affect vertigo?
Conclusion: Reclaiming Your Balance
The moment the world stops spinning is profound. The silence of motion is something you never appreciate until you’ve lost it. Remember, BPPV is a mechanical problem with a mechanical solution. The Foster Maneuver (#3) or the Epley (#1) are your primary tools to fix the glitch in your biological gyroscope.
Don’t let fear of the spin keep you frozen in bed. Test your neck, find your side, and move with intention. If you are still struggling after trying these at home for a week, or if you are worried about the costs of testing, use the checklists above to navigate the medical system smartly. You have the tools to stop the spin—now go use them.
Next Step: If you are currently dizzy, grab a glass of water, sit on the edge of your bed, and perform the simple diagnostic test to see which ear is the culprit. You could be 15 minutes away from relief.
BPPV treatment, vertigo home remedies, Epley maneuver steps, Foster maneuver, dizziness relief