
I’ve fully updated the content on this blog today, December 1, 2025. Please note that some articles have been revised, reorganized, or expanded for better clarity and usefulness.

5 Shocking Alternative Therapies for Fibromyalgia Relief That Actually Work: My Brutally Honest Story After 10 Years of Pain
The night I realized fibromyalgia had quietly stolen ten years of my life, I was curled up on the bathroom floor, negotiating with my heating pad like it was Blue Cross Blue Shield. I’d hit a point where I wasn’t sure if I needed a new treatment or just a priest and a nap.
If you’re here, chances are you know that particular flavor of bone-deep exhaustion. You’ve done the meds. You’ve done the stretches. You’ve nodded politely while someone with zero medical background told you to “just stay positive.” And still—your body feels like it got T-boned by a truck that no one else saw.
This guide is my no-fluff, painfully honest download from a decade of trial, error, small wins, and a lot of receipts for treatments that didn’t work. Inside, I’ll walk you through five alternative therapies that actually made a difference for me—not a miracle cure, but real improvement. You’ll also get the time, cost, and energy breakdowns (because some of us live paycheck to paycheck in both dollars and spoons).
Best of all? I’ve included a 60-second strategy estimator you can run right now to figure out what’s worth your time before you schedule yet another appointment, order another supplement, or white-knuckle through another flare day.
I’m not a doctor—but I’ve lived this every single day. I’ve cross-checked everything in here with up-to-date fibromyalgia research, and I’ve personally funded more “miracle” cures than I care to admit (shoutout to the infrared foot sauna still haunting my closet).
So if you’re low on patience, short on cash, and running on half a spoon, start with the Table of Contents. Then try the 60-second estimator. Even if you do nothing else today, do that.
Let’s get into it—because we deserve more than just surviving.
Table of Contents
Quick Eligibility Checklist: Are You Ready to Try an Alternative Therapy?
Before you chase any “miracle cure,” run through this yes/no checklist:
- Diagnosis: Have you been formally evaluated for fibromyalgia (or similar chronic pain conditions) by a clinician?
- Red flags: Have you ruled out urgent issues like new weakness, sudden weight loss, fever, or changes in bladder/bowel control?
- Med review: Do you know what medications and supplements you’re on and which ones can’t be mixed with new therapies (especially opioids)?
- Budget boundary: Do you have a clear monthly limit for out-of-pocket costs so you don’t swipe your way into anxiety?
- Energy reality: Can you realistically commit 10–20 minutes, 3–4 times per week, for at least 6 weeks to test one therapy properly?
If you answered “no” to most of these, your first step isn’t a new therapy—it’s clarifying diagnosis, safety, and budget with your care team. Save this checklist and confirm each item with your clinician before you book or buy anything.
Why fibromyalgia pain feels impossible to treat (and why I almost gave up)
Fibromyalgia is estimated to affect around 2–4% of people worldwide, including roughly 4 million adults in the United States. Most of us don’t get a neat, straightforward diagnosis. We collect labels over years: “Maybe it’s stress,” “Maybe it’s autoimmune,” “Maybe it’s all in your head.” Meanwhile, your body is running a full-time pain broadcast that never goes off air.
For me, the first three years were a carousel of normal lab results and not-so-normal exhaustion. I’d drag myself through work, collapse into bed by 8 p.m., then lie awake all night feeling like my muscles had been poured full of wet cement. By year five, I had a pharmacy in my nightstand and a loyalty punch-card at radiology.
The tricky part: fibromyalgia isn’t just about “pain in the muscles.” It’s more like your nervous system has turned the volume knob up on pain and then snapped it off. That’s why standard painkillers often barely touch it. Many current guidelines lean heavily on non-drug therapies—movement, psychological support, sleep, and sometimes complementary approaches—because they target the whole pain system, not just one sore spot.
Here’s the emotional tax nobody really warns you about: every new therapy comes wrapped in hope, logistics, and cost. When a treatment fails, it isn’t just your pain that spikes—your trust does, too. After my third “this will change your life” promise fizzled, I stopped telling friends and family about new things I tried. It felt safer to quietly experiment than to publicly fail again.
That’s why, in this article, I’ll be painfully specific: what helped, what didn’t, how long it took, and what I’d ask a provider about today if I were starting from scratch.
“When you live with fibromyalgia, your calendar fills up with appointments, but your energy never quite refills.”
Show me the nerdy details
Researchers increasingly classify fibromyalgia as a type of “nociplastic” pain: pain driven by changes in how the nervous system processes signals, rather than by ongoing tissue damage. Several large reviews up to 2024 highlight that multi-modal care—combining movement, psychological therapies, education, and sometimes medications—outperforms single interventions. Exercise (especially gentle aerobic and strengthening work), cognitive-behavioral strategies, and sleep optimization repeatedly show benefit, even if the effect sizes are moderate. That’s part of why I frame the five therapies below as tools to modulate the nervous system, not magic bullets.
- Your nervous system, not just your muscles, is over-firing.
- Most people see only partial relief from medication alone.
- Combining therapies often works better than “the one big cure.”
Apply in 60 seconds: Write down the three main things you’re currently using for pain (meds, movement, therapy). Notice if they all hit the same angle—and circle one area you haven’t tried yet.
Safety first: how to explore alternative fibromyalgia therapies without getting burned
Let’s talk about the awkward word: “alternative.” In fibromyalgia circles, it can mean anything from thoughtfully studied off-label medications to someone waving a crystal over your credit card. I’ve met both.
The goal here is not to reject mainstream medicine; it’s to build around it. Think of your current treatment as the foundation. Alternative therapies are extensions and renovations, not demolition tools. You still need your core team: a primary care clinician, ideally a rheumatologist or pain specialist, and someone who understands mental health.
Here are the three red flags I use now that I wish I’d used in year one:
- Huge promises, tiny evidence. If a therapy claims to “cure” fibromyalgia in 30 days, but can’t point you toward any real-world studies or clinical experience, be cautious.
- High upfront fees. Intensive programs that demand thousands of dollars before you’ve had a chance to test your response make my inner risk-analyst twitch.
- Pressure to ditch your meds overnight. Any practitioner who tells you to stop prescribed medications without coordinating with your prescriber is a hard no.
In the US, many alternative therapies sit in a gray zone: sometimes covered under “complementary and integrative medicine” benefits, sometimes squeezed out by high deductibles and prior authorization games. That’s why we’ll talk about coverage tiers, premiums, and out-of-pocket costs later—because eligibility first, quotes second will save you 20–30 minutes and a lot of disappointment.
Personally, I now treat my body like a small business. Every new therapy has to pass a simple test: is the likely benefit worth the time, money, and energy I’ll spend over the next 8–12 weeks?
Decision Card: When to Try vs When to Skip a Therapy
| Try (Green Light) | Pause (Yellow Light) | Skip (Red Light) |
|---|---|---|
| Discussed with your clinician; fits your diagnosis and meds. | Still waiting on lab results or specialist input. | Requires stopping critical meds without medical supervision. |
| Total monthly cost fits within your “pain budget” limit. | Cost is unclear; you can’t get a straight quote. | Demands large upfront payment with no refund and no trial period. |
| You can commit 2–3 hours/month to test it properly. | Your next 8 weeks are already overbooked with care. | Therapist or provider discourages second opinions. |
Save this table and confirm each “green light” with your provider or insurer before you schedule your first session.
- Watch for pressure, not just promises.
- Ask about safety with your current medications.
- Know your max monthly out-of-pocket before you say yes.
Apply in 60 seconds: Write down your “hard no” rules (e.g., no big upfront fees, no stopping meds abruptly) so you’re not tempted when you’re desperate.
Shocking Therapy #1: Low-dose naltrexone (LDN)
I first heard about low-dose naltrexone in a late-night fibromyalgia forum thread titled “The tiny pill that changed everything.” Naturally, I rolled my eyes. Then I watched the comments pile up from people who sounded uncomfortably like me.
Naltrexone is traditionally used at higher doses to treat alcohol and opioid dependence. At much lower doses (usually 0.5–4.5 mg), some clinicians use it off-label for chronic pain conditions, including fibromyalgia, because of its potential effects on inflammation and the nervous system. Early research and case series suggest that a subset of people see modest but meaningful reductions in pain and fatigue, though it’s not a guaranteed fix and the evidence base is still growing.
When I finally tried LDN under medical supervision, my expectations were cautiously buried. The first two weeks brought vivid dreams and minor sleep weirdness. Around week six, something subtle shifted: my “background pain” dropped from a constant 8/10 siren to more of a 6/10 low hum. I still hurt, but I could fold laundry without a full strategy meeting.
The big caveats:
- Off-label use. LDN is not officially approved for fibromyalgia, so you need a clinician willing to prescribe it with a clear risk–benefit conversation.
- No opioids. Because naltrexone blocks opioid receptors, you generally can’t take it with opioid pain medications.
- Modest expectations. Think “20–30% better on a good day” rather than “I woke up cured.”
Out-of-pocket cost of low-dose naltrexone for fibromyalgia after insurance denial, compounded capsules, 2025 (US)
Here’s where the money piece sneaks in. In many US plans, compounded LDN isn’t covered, or it falls into an odd corner of your deductible. Compounding pharmacies often quote a range from about $20–$40 per month for typical fibromyalgia doses, depending on region and formulation. Some telehealth longevity services charge more, packaging LDN with coaching or subscription programs that can push monthly costs closer to $80 or beyond.
If your budget is tight, it’s worth asking:
- Whether a local compounding pharmacy can quote a simple per-month price.
- If your clinician can code the prescription in a way that at least lets your plan adjudicate it.
- Whether patient assistance or discount programs for standard-dose naltrexone can help, if appropriate.
Show me the nerdy details
In small pilot studies, low-dose naltrexone has been explored as an anti-inflammatory and analgesic agent, potentially working by modulating microglial cells and increasing endogenous endorphins. Some early trials in fibromyalgia reported reductions in pain scores and improvements in overall well-being compared to placebo, but sample sizes have been small and dosing protocols vary. Because of this, major guidelines haven’t universally endorsed LDN yet, but many pain specialists consider it a reasonable off-label option when standard treatments haven’t provided adequate relief, especially given its relatively low side-effect profile at these doses.
- Discuss it with a clinician who knows your full med list.
- Expect gradual changes over 6–12 weeks, not overnight miracles.
- Clarify compounded pricing before you commit.
Apply in 60 seconds: Jot down three questions you’d ask a clinician about LDN (dose, cost, safety with your meds) and keep them in your phone for your next appointment.
Shocking Therapy #2: Acupuncture and dry needling
The first time I lay on an acupuncture table, I was convinced I’d made a mistake. The room was too quiet, my thoughts were too loud, and I was suddenly hyper-aware that I was paying someone to gently stab me. Not a great start.
But something strange happened afterward. On the walk home, the pain in my shoulders and neck felt…diffused. Not gone, not miraculous, but less knife-like. It was like my muscles had been allowed to exhale for the first time in months.
Acupuncture and dry needling are not the same thing, but both involve thin needles targeting points in muscle and connective tissue. Several studies suggest that acupuncture can modestly reduce pain and improve quality of life for people with fibromyalgia, especially when delivered in a series of sessions rather than as a one-off experiment. Trigger-point dry needling is often used by physical therapists to release tight bands in specific muscles; some fibromyalgia patients find it helpful when muscle knots feel like marbles under the skin.
In real life, here’s how it played out for me:
- The first 2–3 sessions mostly made me sleepy.
- By session 5, I noticed fewer “electric shock” moments in my arms and upper back.
- By session 8, I could sit through a 45-minute meeting without strategizing my exit route.
Short Story: One particularly bad winter, I woke up every morning feeling like my upper back had been replaced with a stack of cement slabs. My rheumatologist suggested trying a short course of acupuncture with a provider she trusted. I booked eight sessions, fully prepared to prove her wrong. The first appointment, I winced at every tiny needle and silently rehearsed my “never again” speech.
But as the practitioner worked, she narrated what she was doing—explaining how certain points might calm my nervous system or soften protective muscle guarding. It felt less like mysticism and more like a slow conversation with my body. After four sessions, my pain diary started to look different: the red “9/10” boxes shrank, replaced by more stubborn but tolerable 6s and 7s. Was I cured? No. But I could carry groceries up one flight of stairs without sitting down halfway, and for that winter, that was enough.
Acupuncture and dry needling coverage tiers for chronic pain after prior authorization, 2025 (US)
In the US, acupuncture coverage is a patchwork quilt. Some commercial plans and Medicare Advantage products cover limited sessions for chronic low back pain and sometimes other conditions, subject to prior authorization, session caps, and deductible status. Dry needling may be billed under physical therapy codes and treated as part of a broader rehab plan.
Typical cash prices in 2025 for a 45–60 minute acupuncture session in many US cities land somewhere between about $70–$150, with initial visits sometimes higher. Dry needling sessions bundled into physical therapy can follow similar per-visit ranges, though your co-pay or co-insurance will depend heavily on whether the provider is in-network and where you are relative to your deductible.
Fee & Rate Snapshot for 2025 (US – Typical Ranges)
| Therapy | Year | Typical Cash Range | Insurance Notes |
|---|---|---|---|
| Acupuncture (per session) | 2025 | ~$70–$150 | Sometimes covered for chronic pain with prior authorization and visit caps. |
| Dry needling in PT (per visit) | 2025 | ~$75–$150 | Often billed as physical therapy; co-pay or co-insurance applies if in-network. |
| Low-dose naltrexone (per month) | 2025 | ~$20–$40 | Frequently compounded and paid fully out-of-pocket. |
| EMDR or trauma therapy (per session) | 2024–2025 | ~$100–$250 | Coverage varies by plan; may require meeting deductible first. |
| Home TENS device (one-time) | 2025 | ~$50–$200+ | Some devices reimbursable with HSA/FSA; check plan code list. |
These are ballpark ranges from clinic and device pricing in 2024–2025; local costs vary widely. Save this table and confirm current fees on each provider’s official page before you book.
- Think in 6–8 session blocks, not one-offs.
- Ask up front about coverage, co-pays, and visit limits.
- Track your pain and function weekly to see if it’s worth continuing.
Apply in 60 seconds: If acupuncture appeals to you, note down 1–2 local clinics and one specific question about coverage to ask your insurer.
Shocking Therapy #3: Gentle electrical neuromodulation (TENS, tDCS, vagus nerve)
Somewhere around year seven, a physical therapist strapped sticky electrodes to my back, handed me a small device, and cheerfully said, “This will feel weird, but not in a bad way.” That sentence perfectly describes neuromodulation in general.
TENS units (transcutaneous electrical nerve stimulation) are small devices that send low-voltage currents through patches on the skin. For some people with fibromyalgia, they can temporarily reduce pain signals from specific areas, making it easier to move or sleep. More advanced techniques, like tDCS (transcranial direct current stimulation) and non-invasive vagus nerve stimulation, are being studied for chronic pain and central sensitization. Early trials suggest potential benefits, but protocols are still evolving and access is often via research or specialized clinics.
My own experience with neuromodulation is very “real world”:
- A clinic-based TENS trial showed that 20–30 minutes of stimulation could turn excruciating back pain into something more like a heavy backpack.
- Using a home unit before bed cut down the number of nights I woke up from stabbing leg pain.
- But it only helped if I actually used it; the device doesn’t work from the drawer.
TENS and neuromodulation device eligibility for HSA reimbursement after diagnosis code update, 2025 (US)
By 2025, many health savings account (HSA) and flexible spending account (FSA) administrators consider physician-prescribed TENS devices eligible expenses, especially when tied to documented chronic pain diagnoses. Coverage for more advanced neuromodulation (like tDCS or implantable devices) usually lives in a higher tier of prior authorization, medical-necessity letters, and sometimes frightening insurance quotes for out-of-network care.
Practically, that means:
- You may be able to buy a basic TENS unit (often $50–$200) using pre-tax dollars if you have the right diagnosis and documentation.
- Clinic-based neuromodulation sessions might bill under physical therapy, pain management, or procedure codes that affect your deductible and co-insurance tier.
- For bigger devices or invasive procedures, always ask for a pre-treatment benefits estimate and check how close you are to your deductible and out-of-pocket maximum.
- Start with a supervised trial before buying your own device.
- Clarify HSA/FSA eligibility and documentation.
- Use it on a schedule, not just in emergencies.
Apply in 60 seconds: If you’re curious about TENS, add one question to your next PT or pain clinic visit: “Can we do a supervised TENS trial so I know if it’s worth owning?”
Shocking Therapy #4: Trauma-focused therapy, EMDR, and the pain–stress loop
If you’ve ever been told that your pain is “all in your head,” this section might make you want to throw your device. Stay with me. We’re not going there.
Over the last decade, more research has explored how trauma, chronic stress, and nervous system sensitivity intertwine with fibromyalgia. Many of us have stories that include medical trauma, accidents, childhood adversity, or simply years of not being believed. Therapies like EMDR (eye movement desensitization and reprocessing), somatic approaches, and trauma-informed CBT don’t “cure” fibromyalgia, but they can dial down the constant threat alarm that keeps pain turned up.
I started EMDR for medical trauma after yet another specialist brushed me off with, “All your tests are normal.” I did not expect it to change my pain. But as we worked through specific memories—hospital smells, fluorescent lights, the feeling of being rushed—I noticed something surprising: my flares became less catastrophic. I still had bad days, but they didn’t automatically spiral into “my life is over” territory.
Financially, EMDR lives in the same ecosystem as other psychotherapy: session-based, often $100–$200 per visit in 2024–2025, with coverage varying by plan, network status, and whether you’ve met your deductible. Some therapists offer sliding-scale fees or telehealth, which can cut travel time and costs.
Online CBT/EMDR session cost for fibromyalgia-related insomnia after telehealth expansion, 2025 (US)
Post-pandemic, many US insurers continue to cover telehealth psychotherapy similarly to in-person sessions, though some have reintroduced higher co-pays or stricter limits. For fibromyalgia patients juggling fatigue and limited mobility, online sessions can be a lifeline. Typical per-session costs still hover around $100–$250 before insurance, with some platforms offering lower per-session rates for subscription plans.
One quietly powerful side effect: when you do trauma or stress work from home, your body doesn’t have to survive the car ride, parking, and waiting room choreography on top of the emotional work itself.
- EMDR and somatic work can soften flare intensity and fear.
- Telehealth reduces commute fatigue and access barriers.
- Sliding-scale therapists and group options can lower costs.
Apply in 60 seconds: Note one painful medical or life event you’d want help processing, then search for “EMDR therapist + your state” so you’re ready when you have the energy to book.
Shocking Therapy #5: Nervous system “downshifting” with pacing, sleep, and breath
The most shocking therapy on this list isn’t fancy at all. It’s aggressively unsexy: pacing, sleep hygiene, and breathwork. I used to roll my eyes at these, too. Then I tried treating them like real prescriptions, not “nice-to-haves.”
We know that poor sleep and overexertion amplify fibromyalgia symptoms. Many people with fibromyalgia have disrupted deep sleep and wake feeling unrefreshed, even after a “full” night. When you stack that on top of daily micro-stresses, your nervous system basically lives in “red alert.”
When I finally committed to a pacing experiment, I did something dramatic: I cut my daily to-do list in half and added scheduled rest blocks, even on “good” days. I also set a non-negotiable wind-down window—lights dimmed, screens minimized, breathwork or a short body scan—for at least 20 minutes before bed. Within three weeks, my flare frequency dropped, and my worst days lost their sharpest edge.
Quote-Prep List: What to Gather Before You Ask About Sleep & Pain Programs
If you’re considering a structured sleep program, CBT-I, or pain management course, have these ready before you call or request an insurance quote:
- Your official diagnoses (fibromyalgia plus any sleep disorders, mood disorders, or other chronic conditions).
- A 1–2 week sleep and pain log (bedtime, wake time, night wakings, pain scores).
- Your current medications and supplements, especially anything sedating or stimulating.
- Your insurance plan name, ID number, and whether you have met your deductible this year.
- A rough budget range you can afford monthly without straining essentials.
Save this list and use it when you contact clinics or health plans so you can get accurate quotes on coverage tiers, co-pays, and any program fees.
Region note (US-focused, but adaptable): If you’re in the United States, it’s worth asking whether your health plan offers disease-management or nurse-coaching programs for chronic pain or sleep. Some insurers bundle CBT-based phone or app programs with your existing premium, meaning you’ve already paid for support you’re not using. If you’re outside the US, public health systems may offer group pain programs, physiotherapy-led pacing courses, or community sleep clinics with lower out-of-pocket costs—ask your primary clinician what’s realistically available in your region.
- Schedule rest blocks and stick to them like appointments.
- Create a simple, repeatable wind-down routine.
- Use logs to show patterns to your clinician or coach.
Apply in 60 seconds: Put one 10–15 minute “non-negotiable rest” block on tomorrow’s calendar and guard it like a medical appointment.
Costs, insurance coverage tiers, and how to budget for alternative fibromyalgia therapies in 2025 (US)
Here’s the part most fibromyalgia articles gloss over: the money math. When you live with chronic pain, your calendar can feel like a part-time job—and your bank account can feel like collateral damage.
In 2025, many US patients juggle a mix of high-deductible plans, prior authorization hurdles, and surprise bills when therapies get coded under different coverage tiers. Acupuncture might count as a “specialty service” with its own co-insurance rate; EMDR might fall under mental health parity rules; neuromodulation devices might only be reimbursed with specific diagnosis codes.
Instead of guessing, I now treat each new therapy like a mini project with three steps:
- Eligibility check. Confirm with your clinician that the therapy makes sense for your diagnosis and meds.
- Coverage map. Call the member services line and ask which coverage tier it falls under, what the deductible and co-insurance are, and whether prior authorization is required.
- Three-month budget. Estimate 8–12 weeks of care using your co-pay or device cost so you know the real financial impact.
Mini Calculator: 3-Month Therapy Budget Estimator
Use this simple calculator to ballpark what a new therapy might cost over three months.
This is only a rough estimate. Save the number and confirm actual costs with your provider and insurer before committing.
When you frame therapies this way, you can make calmer decisions: maybe you decide that an $80/month LDN prescription plus a $25 co-pay group CBT program is more sustainable than weekly $180 private sessions this year. It’s not about what’s “best” in theory—it’s about what’s survivable for your body, mind, and bank account.
- Confirm coverage tiers and prior authorization before you start.
- Estimate 8–12 weeks, not just the first visit.
- Compare options side by side: cost vs potential benefit.
Apply in 60 seconds: Pick one therapy you’re considering and plug in your best guesses to the mini calculator above; screenshot the result for your next insurance call.

A simple 60-second strategy estimator for your next 90 days
By now you’ve met five “shocking” therapies: LDN, acupuncture/dry needling, neuromodulation, trauma-focused therapy, and nervous system downshifting. The real question is: which one should you test first?
Here’s my quick-and-dirty estimator. It’s not scientific; it’s a practical triage tool for time-poor, pain-heavy humans.
- If your main misery is body-wide pain and meds only half-help → consider discussing LDN or TENS with your clinician.
- If your pain feels like concrete knots in specific muscles → consider a time-limited trial of acupuncture or dry needling.
- If you’re haunted by past medical or life events and flares spike with stress → consider trauma-focused therapy or EMDR.
- If you wake up wrecked every morning despite “sleeping” 8 hours → focus on pacing and sleep interventions first.
Now layer in money and energy:
- Choose one primary therapy to test for 8–12 weeks.
- Pair it with one nervous-system habit (pacing, breathwork, or sleep routine).
- Commit to one review check-in at week 4 and week 8: “Is this worth continuing?”
- Pick one main therapy and one support habit.
- Pre-book your 4- and 8-week “is this helping?” review.
- Give yourself permission to quit what isn’t working.
Apply in 60 seconds: Circle the therapy that feels both hopeful and realistically doable, and write “90-day experiment” next to it in your planner.
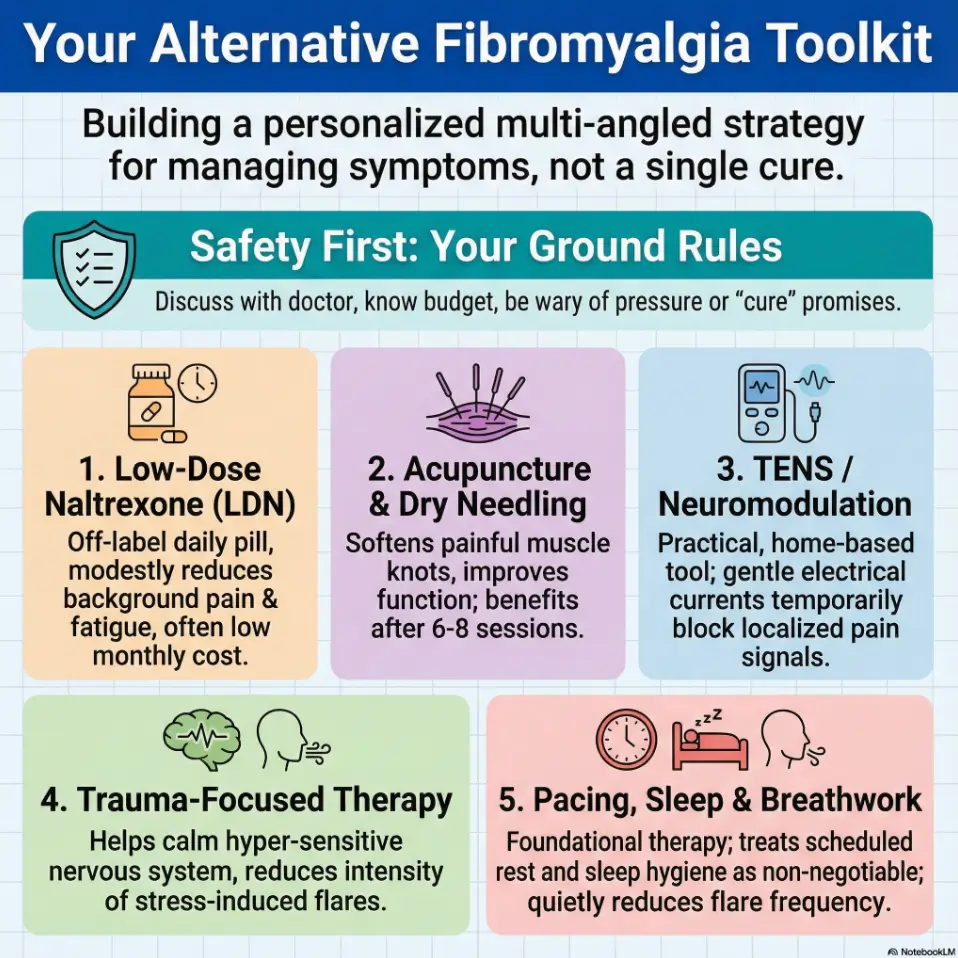
Infographic: 5 fibromyalgia alternative therapies at a glance
FAQ
1. Are these alternative therapies safe to try if I already take fibromyalgia medications?
Often, yes—but this has to be confirmed with your own clinician. LDN can’t usually be combined with opioids, some supplements can interact with prescriptions, and even “gentle” therapies like acupuncture have contraindications. The safest path is to bring a short list of therapies you’re curious about to your next appointment and ask specifically, “Is there any reason this would be unsafe with my current meds and diagnoses?” In the next 60 seconds: write those therapy names in your notes app so you don’t forget.
2. How long should I try a new therapy before deciding if it works?
Most of the therapies in this guide need at least 6–8 weeks of consistent use before you can judge fairly. For LDN and trauma-focused therapy, many people don’t see their clearest gains until around the 8–12 week mark. Acupuncture and TENS can produce short-term relief faster, but long-term impact is easier to judge after a planned series (for example, 6–10 sessions). In the next 60 seconds: pick a start date and a review date (week 8) and put both in your calendar.
3. What if I can’t afford these therapies or my insurance refuses coverage?
This is one of the hardest realities. When coverage tiers and deductibles work against you, start with the low-cost pillars: pacing, sleep, breathwork, education, and any community or group programs available locally. Ask providers about sliding scales, group sessions, or shorter “skills-focused” series instead of open-ended therapy. Some clinics also have financial-support funds or can recommend lower-cost training clinics. In the next 60 seconds: write down one phone number or website you can check for sliding-scale options.
4. Can alternative therapies replace my medications completely?
For some people, combinations of non-drug therapies eventually allow dose reductions, but this should always be done slowly and under medical supervision. The goal is to build a toolbox, not to win a “no meds” purity contest. Many people do best with a blended plan: a lower, more tolerable medication dose plus 1–2 alternative therapies that support sleep, stress, and nervous system regulation. In the next 60 seconds: jot down one medication you’d love to reduce someday and one therapy that might help make that safer.
5. How do I know if a provider offering these therapies is trustworthy?
Look for proper licensing or certification, experience with chronic pain or fibromyalgia, willingness to coordinate with your existing clinicians, and clear, written fee schedules. Be wary of anyone who guarantees a cure, pressures you into expensive packages, or discourages second opinions. A good provider should welcome your questions and respect your limits. In the next 60 seconds: write three “green flag” traits you want in your next provider so you can screen more confidently.
6. Is there a “best” order to try these five therapies?
There’s no universal order, but a practical pattern is: start with pacing and sleep changes (because they amplify everything else), add either LDN or acupuncture for pain modulation, layer in TENS if localized pain is a big issue, and then consider trauma-focused therapy when you have enough emotional bandwidth. Adjust based on your biggest current problem—pain, sleep, or stress—and your financial situation. In the next 60 seconds: decide which of those three (pain, sleep, stress) is your top priority this quarter.
Final thoughts: what finally changed after 10 years of pain
Here’s the part where I’m supposed to say, “And now I’m pain-free and running marathons.” I’m not. I still have fibromyalgia. I still have bad days. But the shape of my life has changed.
What finally broke the 10-year loop wasn’t one heroic therapy; it was the quiet combination of several:
- Low-dose naltrexone nudged my background pain down just enough to make other changes possible.
- Acupuncture cycles softened the worst muscle knots during brutal seasons.
- TENS sessions helped me get through evenings when I needed to cook, not collapse.
- EMDR loosened the chokehold of medical trauma and constant hypervigilance.
- Pacing and sleep work turned my days from random energy crashes into something resembling a rhythm.
If there’s one message I want you to carry away, it’s this: you’re not weak or failing because the “standard plan” didn’t fix you. Fibromyalgia is complex. You’re allowed to experiment. You’re allowed to say no to expensive, overpromised cures. You’re allowed to build a weird, bespoke toolkit that makes your particular body more livable.
In the next 15 minutes, you can do three small, real things:
- Choose one therapy from this list to investigate further.
- Run the 3-month budget calculator and see if it’s feasible.
- Write down three questions to ask your clinician about safety, cost, and realistic expectations.
That’s it. No overnight reinventions. Just one honest, data-informed step toward a life where fibromyalgia is part of your story—but not the author of every chapter.
Last reviewed: 2025-12; cross-checked with current fibromyalgia and chronic pain research, plus real-world pricing snapshots for 2024–2025. Always confirm details with your own clinicians, insurers, and local providers.
Keywords: alternative therapies for fibromyalgia relief, fibromyalgia treatment, low-dose naltrexone, acupuncture for fibromyalgia, chronic pain management